
I am an IBCLC (International Board Certified Lactation Consultant) in private practice in Northern Ireland and a La Leche League Leader with La Leche League of Ireland
It Hurts! Moving towards Comfortable Breastfeeding
The next blog in our series looking at the first week is on Sore Nipples / Painful Breastfeeding. The 2010 UK Infant Feeding Survey lists "having painful breasts or nipples" as the reason that 22% of women in Northern Ireland who start breastfeeding have stopped within the first week. There's a lot of conflicting information that reaches pregnant mums around this issue and I have heard many pregnant mums here in NI say they have heard that breastfeeding is painful. Is this surprising when 22% of their friends /family who started breastfeeding stop for that reason? Despite this, antenatal literature and breastfeeding support sites commonly state that breastfeeding should never be painful, and if it is something is wrong. So how does this set our expectations?
What is the reality?
Antenatal educators walk a very fine line in trying to prepare mums with accurate expectations, and yet trying to give very positive information. They are trying to cater to all women, and different women want different information. Some want to know everything so they can be prepared for all possibilities, and some would rather just deal with any obstacles as they arise. Often breastfeeding educators often don't want to say anything negative at all, in case they discourage women who are 'on the fence' about how to feed their babies. The fact is that those women are hearing information from society at large though. I think on the whole, I hear more mums say they wish they had known more about what to expect so I am going to try to be as honest as possible on the early days.
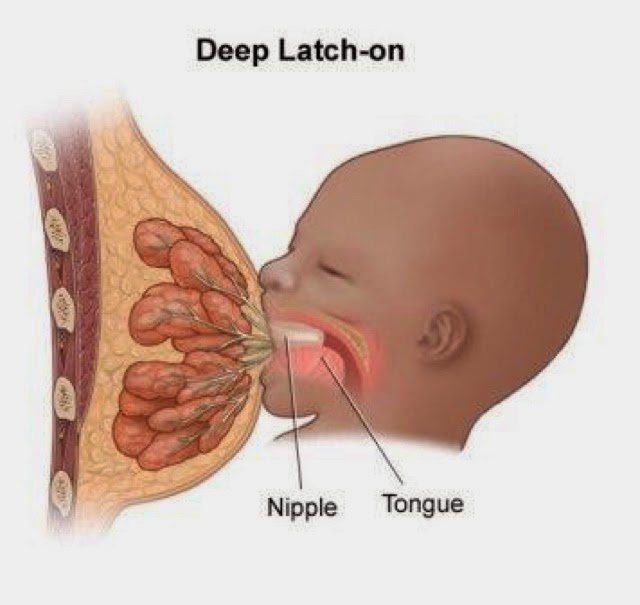
When a baby is latched on well, mum's nipple is in a part of the mouth known as "the comfort zone". The areola and breast underneath mum's nipple is within baby's mouth and her nipple is drawn far back towards his soft palate. When against the soft palate mum's nipple is surrounded by soft tissues and feeding is comfortable and painless. In order to reach the comfort zone, mum's nipple is stretched quite far into her baby's mouth. In fact her nipple stretches to over twice its normal length.
Most new breastfeeding mums do experience some pain in the first few days. Even with what looks like a perfect latch many new mums do experience pain. I have never found anything completely definitive on the cause, but I favour a suggestion that it may be due to this stretching of the nipple. Most of us have never had our nipples stretched to that degree prior to breastfeeding, and it requires the ligaments behind the nipple to stretch. If we stretched the ligaments of any other part of our body to twice their normal length we would expect to feel it! Why should a nipple be different? The absolute key point to this is that it happens in the early days only. Most new breastfeeding mums experience some pain in the first DAYS. This pain is only when baby latches and draws the nipple in. It lasts a few seconds. I will say that again - it lasts a few seconds within the first few days! It should not last for the duration of the feed, and within a few days (for most it is less than a week) the latch pain is gone and breastfeeding should be entirely painless from start to finish. Perhaps the ligaments have loosened a little by this point.
Some sources suggest the pain is due to the milk ducts being used for the first time, and the reason that the pain disappears after a few seconds is because the milk begins to flow more quickly.
If the pain is lasting more than 30 seconds into a feed then it is likely that your nipple is not in the comfort zone and the latch should be adjusted. Some breastfeeding support professionals will suggest that you unlatch and relatch at this point. Other professionals suggest you should try to adjust baby's latch mid-feed in order to avoid the latch pain another time. (see the links at the end of the blog). Whichever way you decide to approach it, do not continue through a feed with a painful latch. Don't be tempted to think, "well, it's a bit uncomfortable but it will probably be ok". It should be painless after the initial latch - entirely painless. If it is uncomfortable it is likely that the latch is not deep enough. That means your nipple may be compressed against the hard palate of your baby's mouth rather than the soft palate, and that actually causes trauma - grazes and cracks. Grazes and cracks are common in the early days but can be avoided entirely with a good latch. Everything comes back to the latch. In the comfort zone your nipple is safe, and without any compression or friction any grazes or cracks heal incredibly quickly.
Can you do something to prepare your nipples before giving birth?
Years ago women were advised to "toughen up" their nipples before birth, with weird suggestions like using methylated spirits, or brushing the nipples. Ouch! I can kinda see where these ideas came from, but nipples don't get tougher during breastfeeding! They perhaps get more stretchy, but not tougher. No preparation is needed. Just as no preparation is needed for your cervix to dilate or your perineum to stretch for you to birth your baby, no preparation is needed for your nipples.
Perhaps we should consider birth as a process rather than a event that ends when a baby is born and the cord cut. Birth is not just about a baby. It's also about the birth of a mother and it can help to think of her birth like a contraction - with a building stage, a peak and an easing off. The build up may have a period of Braxton hicks or pre labour etc, reaching a peak where she labours and birthes her baby. The easing off period involves after pains of her uterus contracting and the beginning of breastfeeding. Mums who choose not to breastfeed still produce milk in the early days, and without breastfeeding to remove the milk they feel the pain and discomfort of engorgment which lasts throughout the day, rather than for a few seconds at certain times of day. For those who do breastfeed, the afterpains of both the uterus and nipples ease and resolve within days and the breastfeeding mother has been born!
When pain is not normal
I do want to emphasis is what is normal and to be expected, and what requires help. Initial latching pain/discomfort is normal. It should last less than 30 seconds in any feed and be gone completely in a few days just as the uterus afterpains are. Just as those uterus afterpains can be managed, so can the latch. Some mums will use painkillers, and some will use their labour breathing techniques.
If pain is lasting longer than 30 seconds, or is not improving after the first week this is not normal and suggests the latch could be adjusted. Cracks and grazes are not normal and need treated; care also needs to be taken to adjust the latch. Any pain between feeds, pain within the breast, redness or feeling of heat in the breast is not normal and needs assessed. Your midwives (hospital or community) can help you with the latch and with information around any adjustments or treatment. You can also contact your local breastfeeding support groups who will have a trained breastfeeding counsellor /lactation consultant who can support you with latch and treatment information.
How will I know if the latch is ok?
Getting a good latch is the key to easy breastfeeding. There are lots of articles online and in print about how you can assess a good latch, like your Off To A Good Start booklet (for NI readers). They summarise points like these - there should be more areola visible above the nipple than below, baby's mouth should be wide and lips flanged, baby's chin should be against the breast and his nose should be off the breast. Those are good guidelines to check your latch against. Ultimately though, you will know that you have a good latch if feeding is comfortable after the first few seconds. The previous blog talks about how to use your instinctive reflexes to help get a good latch right from the start.
Using the biolgical feeding position will help enormously. If you choose not to use this position and are holding your baby across your chest remember to support your baby's neck and shoulders rather than holding his head. If you hold his head he is unable to tilt his head back and get a wide gape. Pregnant mums in NI have seen a lot of bottle feeding, but not so much breastfeeding. Latching to a breast is different than latching to a bottle. Don't be tempted to treat your breast as a bottle and to place your nipple in your baby's mouth. Line up your baby's nose to your nipple keeping his chin into your breast. It will look like he can't reach your nipple with his mouth, but he will! In this position he can tilt his head back and reach forward to get a nice deep latch. He needs to be in this position to get plenty of breast below the nipple into his mouth. This is the key to a deep latch and to breastfeeding, rather than nipple feeding. There are diagrams and videos showing a good latch in the further information section below which will help, as will getting to a local breastfeeding support group and a good antenatal breastfeeding class.
Healing sore nipples
There are lots of really good resources on healing sore nipples on the web, so I have put them in the further information section rather than trying to reinvent the wheel. The most important part of healing any trauma is getting the latch right. Once you correct the latch and have your nipple in the comfort zone your normal healing processes resolve any cracks and grazes very quickly. If you don't correct the latch you nipple continues to have friction which means any grazes take much longer to heal.
A quick note on lanolin! Nipples heal more quickly if kept slightly moist - to prevent any cracking. Some mums will use lanolin for this, some will use proprietary compresses available from pharmacies, some will use something like coconut oil. I often hear mums talk about how helpful lanolin is and suggesting that new mums "slather it on" liberally before or after feeds. I think there is a lot of confusion in the community about the role of lanolin. Lanolin is a wax secreted by sheep on to their wool. In breastfeeding it is used to stop a damaged nipple from drying out. It does not heal cracks (your body heals the crack), and it isn't a cure for a latch problem. Using a lot of lanolin (or any other slippy substance) before feeds actually makes your breast slippy and that makes it harder for your baby to breastfeed well. If you choose to use lanolin to help with cracks, it is only used after feeds until the nipple has healed. Then it is no longer needed. It is not an essential piece of breastfeeding equipment and many breastfeeding mums never use lanolin.

If you need some help correcting a painful latch contact someone who can help ASAP. The sooner it is done the quicker you will heal, your baby will be able to transfer milk more easily and the easier breastfeeding will become. An upcoming blog will look at who provides breastfeeding support in NI, but for now your local options in the first week are your community midwife, your local peer support mums, voluntary breastfeeding support organisations like La Leche League, or a lactation consultant (IBCLC).
Remember that your birthing latch pains should ease and be entirely gone within a few days of the birth of your baby and then feeding should be entirely painless from start to finish. Not only painless, it should be enjoyable, pleasant and relaxing. Within a short time latch pain is completely forgotten, and just like labour pain we move into a kind of amnesia that it ever existed... And that's as it should be. With so many reasons why we should breastfeed, it just makes sense that nature dissolves the memory away into a forgotten haze and leaves us instead with the beautiful bonding experience that is comfortable breastfeeding.
If you have any questions about a consultation or would like to arrange to meet, please get in touch.
Important Information
All material on this website is provided for educational purposes only. Online information cannot replace an in-person consultation with a qualified, independent International Board Certified Lactation Consultant (IBCLC) or your health care provider. If you are concerned about your health, or that of your child, consult with your health care provider regarding the advisability of any opinions or recommendations with respect to your individual situation.