
I am an IBCLC (International Board Certified Lactation Consultant) in private practice in Northern Ireland and a La Leche League Leader with La Leche League of Ireland
What is a Nipple Shield & Why would I use it?
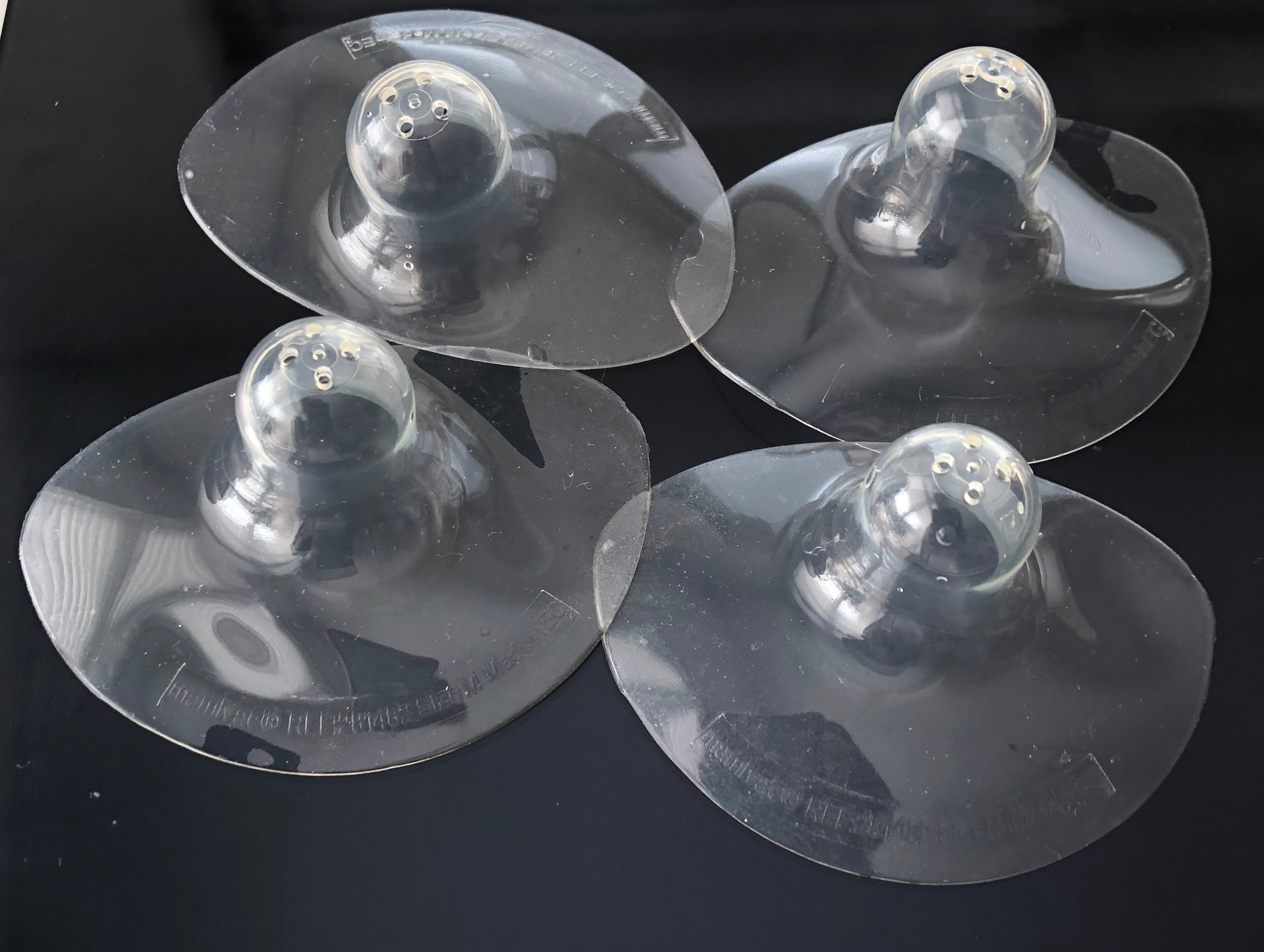
A nipple shield is a thin silicone nipple with a larger diameter silicone base. A shield is often used short term to overcome breastfeeding problems and sits over the nipple and a small area of the breast around the nipple. The shield has a series of small holes on the end of the nipple area allowing to milk to transfer through. A breastfeeding baby can then latch directly to the breast and feed with the shield forming a kind of passive intermediary role between the nipple and the baby's mouth.
According to the literature, shields in one form or another appear to have been in use as early as the 1600s and have been made of a very wide variety of materials over the years (silver, wood, wax, wood, lead, tin, bone, horn, ivory, glass, pewter, gum elastic) - essentially anything that could be moulded into generally the right shape. The rigid versions must have been pretty difficult for a baby to use as it would have made it impossible for the baby's tongue to directly stimulate or "work" the breast, and thankfully modern silicone versions are very thin, flexible and allow good sensation on the breast.
Shields are used for a wide variety of reasons. A study of 202 breastfeeding mothers in the US (Powers & Tapia 2004) found that mothers used them for the following reasons:
- Flat or inverted nipples (62%) - It is obvious how a shield helps with this situation. The shield creates and maintains an evert nipple shape for the baby to latch on to.
- Disorganized suck (43%) - This phrase covers a multitude of different issues - essentially anything which deviates from what we expect of a good attachment and sucking pattern in the full term healthy newborn. It could be a baby who can't latch on / who latches but doesn't suck / who latches and instantly falls asleep / who sucks but doesn't transfer milk well / who sucks but can't maintain the attachment and falls off / who latches and sucks but can't coordinate the whole process well. Just as it causes many different issues, these can have multiple causes! It may be due to pain relief drugs during labour / instrumental or traumatic birth / medical conditions causing low muscle tone to name a few. Nipple shields can help to compensate for the sucking issues by maintaining a firm evert nipple shape in the baby's mouth and creating some protection for the nipple from the disorganised movement.
- Sore Nipples (23%) - This is a very common reason for short term use in the early days in my experience. Where, for example, breastfeeding has been painful in the early days, and perhaps there is nipple trauma, using a shield is a relatively common suggestion. In this case the shield provides a barrier between the sore, traumatised nipple and the baby's mouth. It allows us to keep breastfeeding but creates a "safety" barrier preventing direct friction to the nipple. It provides some space, both physically, psychologically and creates some time space to work on getting a deep attachment without more trauma. In this case it is usually used for a few days or maybe a couple of weeks and then removed again.
- Engorgement (15%) - In the early days it is very common to experience some engorgement where the breasts become overfull and distended with milk and fluids. When this occurs the nipple can appear flatter against the breast, and the breast can be so firm/hard that the baby finds it difficult to latch on deeply or get much breast tissue into the mouth. Nipple shields would not be my preferred resolution in this situation, as there are lots of other techniques to help the baby to latch directly to the breast, such as reverse pressure softening, but shields can help a baby at the breast in this situation until you get the support you need to latch without them.
- Prematurity (12%) - In order to breastfeed effectively babies need to be able to cup their tongue around the breast, pull the breast into their mouth, maintain the seal with lips and tongue, create vacuum, perform a peristaltic tongue action and coordinate their suck, swallow and breathe rhythm. It's a fairly complex sequence and premature babies can have a number of challenges. Depending on their gestational age babies may have an immature, disorganised suck. They also lack the good fat pads in the cheeks that full term babies have, and that can make it more difficult for them to create vacuum. They can also tire easily, and be unable to maintain a deep attachment. Nipple shields can compensate for many of these issues. The shield creates firm pressure in the mouth with a nipple which stays evert without the baby needing to maintain vacuum or tongue cupping. Many premature babies really benefit from shields
- Tongue Tie (1%) - This category could just as easily be placed under Disorganised Suck and/or Sore Nipples, as a tongue restriction prevents the tongue from moving normally. It may cause pretty much all the issues listed in that category - inability to latch, or to latch deeply, or maintain attachment, or to transfer milk effectively etc, and the lack of deep attachment and correct tongue movement means there is often friction causing pain/trauma to the nipples. Nipple shields can help by compensating for the baby's disorganised suck and can also create a barrier around the nipples so reducing the friction and trauma and can, for some babies, help keep baby at the breast until the tongue tie is released.
Another use, not listed in this study is as a transition tool from bottle to breast. Shields are sometimes used to help a baby who is used to feeding from bottles to transition back to the breast if they are not latching on. They can create a similar mouth feel to the bottle, and so are familiar and once baby is transitioned to the breast with the shield, then the transition to the breast without the shield can be worked on.
How Common is Using Nipple Shields?
In my view, it's pretty common at least temporarily. I don't have figures however. I did do a quick literature search of studies on nipple shields looking for this. I couldn't find any studies looking at the prevalence of nipple shield use. Lots of papers discussing whether they are helpful or a problem, whether they impact milk transfer or milk production, but none looking at large numbers of breastfeeding dyads and checking prevalence of nipple shields. In my own private practice and in my volunteer work however I see them very often - usually often only for a few days but sometimes for very long periods - months, or even into the 2nd year. Almost without exception though when someone tells me they are using shields it is with a sense of reservation - a little fear of judgement of using them, that they feel I will say they shouldn't use them or that I will caution them about problems they will cause. Often they have either read or been told that they impact milk supply, or that they mean that the baby will not be able to feed without them, or they will find it hard to get rid of them again, or that they can only use them short term. They seem (at least locally) to hear only information cautioning against them, and less information discussing whether they could be helpful in some circumstances, and whether the concerns are justified.
Are Shields a Help or a Hindrance?
My take on shields is that they are a tool. Whether a tool helps or hinders depends on how you are using it, whether it is appropriate to use, how you feel about it, what your long term goal is, whether that tool helps you to reach that goal, and whether you can minimise any risks that tool might pose to your ultimate goal. So, let's look at a few of the common concerns and what the research says about shields.
Impact on Amount of Milk the Baby Drinks
There are certainly studies showing that babies drink less milk when using shields. Some of these studies are as much as 30 years old, with shields of older thicker construction (such as rubber) or experimental use with babies who don't normally use nipple shields. This certainly should give us pause for thought, but there are more recent studies which show different results. A 2009 study (Chertok et al) looked at 54 babies who were regularly using nipple shields. The mothers were not expressing milk after feeding. They found no significant difference in weight between the babies using a nipple shield and the babies who were not. This would suggest that the babies were getting adequate milk and the breasts were being stimulated well through the nipple shield.
There are even some studies showing preterm babies may drink more when they breastfeed using a shield compared to when they breastfeed without a shield. Meier et al, 2000, found that preterm babies using a shield drank on average half an oz (14.4ml) more when using a shield, they stayed awake for longer at the breast and had longer sucking bursts. On average they used shields for 32 days, and there was no association between the length of time a shield was used and the total length of breastfeeding. In other words using a shield had no effect on how long a dyad breastfed for - it didn't seem to cause any early weaning. This study seems to back up an earlier 1996 study (Clum & Primomo, 1996) which found that 9 out of 15 preterm infants consumed 50% more milk when using a shield.
Impact on Hormone levels (Stimulation of Breast)
Part of the reason that women have often been encouraged to express after each feed when using a nipple shield is due to a concern that the breast would not be adequately stimulated when there is a barrier on the breast. An 1987 study (Amatayakul et al) however, found this not to be the case. They found that both prolactin and cortisol levels were not significantly different between those using shields and those feeding directly at the breast. This study was one which found the babies drank less milk however, so they did suggest that perhaps this was due to a change in oxytocin release (and that would potentially affect letdown / milk ejection). Oxytocin was not measured however, and this was using a thin latex shield. Modern shields are more commonly made of silicone, so it is unclear if this makes a difference. The study by Chertok et al (2006) of 32 mothers found that there was no significant difference in either hormone levels or milk intake when using an ultrathin, flexible shield.
Baby will not learn to breastfeed without the shield?
Some women are told not to use shields as their baby will never learn to breastfeed without them - or that they should only be used for a few days otherwise they will never wean off them. This is not what the research or my clinical experience would suggest for the most part. The Meier study (2000) mentioned above found that the preterms transitioned well from shields (Average 32 days of use) once their suck was better developed. A US study looking at dyads who had used shields found that 67% of them weaned off successfullly (Powers & Tapia 2004). The remaining 33% continued to use shields for the entire length of time that they breastfed but 11% of these said that their baby would actually have breastfed without it. They chose to continue using the shield as breastfeeding was more comfortable for them while using it. That leaves only 22% of people who were unable to breastfeed without the shield. It is not clear if those reasons were due to the original difficulty which lead to use of shields (e.g. disorganised suck / tongue tie etc) or whether it was due to the baby not wanting to feed without the shields.
A study in private practice (Bodley & Powers, 1996) reviewed 10 women who used a shield beginning in the first 18 days after birth. Some used them for less than 6 months, the longest was 3.5 months. 9 out of 10 of the babies transitioned to feeding directly from the breast. The 10th switched to bottle feeding due to issues with weight gain. Most babies will wean from shields, but it is true that some people use them for the entire duration of their breastfeeding.
Nipple Shields can Preserve Breastfeeding
Nipple Shields can absolutely be a help for mums - for many reasons. I know very many people who will say that breastfeeding is what allowed them to continue. They either allowed them to get over a short term difficulty (early day problems usually) or allowed them to continue feeding when they would otherwise have stopped. The research also backs this up and also often describe positive experiences in those using shields. Powers & Tapia (2003) asked women, "Do you feel the nipple shield helped you to succeed at breastfeeding?" 88% of the women answered Yes. In addition 98% of them said that if they needed to use shields again with another child they would do it.
A recent 2016 study (Kronberg) did find a 3 times larger risk of stopping breastfeeding when using shields, but also found that of the almost 5000 mothers interviewed those using shields tended to have babies of lower gestational age (more likely to be premature) and lower birthweight and these babies may have had a higher risk of weaning earlier even if not using shields due to feeding issues.
Choosing & Using
There are slight variations in shield design and also in shield size. Firstly there are 2 main shapes of nipple. There are conical shields, and cherry shields. The names are fairly self explanatory and refer to the shape of the nipple (in the same way that pacifiers have different shapes. Conical shields are more readily available in shops locally in my experience, and are fine for most babies. Cherry shaped can help some babies with greater difficulties.
The next set of variations is in the shape of the silicone section which sits over the breast. Some have a circular area of silicone, some have a cut out area where baby's nose should be (which prevents the silicone folding back over baby's nose while feeding). The best shape for you can depend on your breast shape. If your nipples are quite low on the breast for example the cutout shield may be better as a round shield may not maintain good contact under the nipple. If your nipple is higher it's likely that either shield is a valid option.
The last variation is the number of holes which may vary from 3 to 5. Smaller numbers will likely slow the flow more than a shield with more holes - although I don't believe any research has been done on this and looking at impact on milk transfer.
Sizing
Nipples can vary remarkably in size and shape and having a nipple shield that fits is important. The size refers to the base of the nipple, and shields will vary in size from 18mm to perhaps 28-30mm. In practice most local pharmacies or supermarkets are unlikely to have a wide range of sizes, and generally will stock an average nipple size or perhaps will have a couple of sizes based around the average. Getting the right size of shield for you and your baby are important for making sure there is adequate milk transfer to the baby. If the nipple part of the shield is too large /long for your baby they may have difficulty with latching deeply on to the shield. In order to make sure that the baby is feeding well from a shield we need to make sure that they get latched on deeply and the latch looks similar to how it should look directly at the breast. A large shield may not allow the baby to latch deeply and your baby's lips may end up around the nipple part of the shield instead of being on the breast. That could easily lead to less milk being drunk and lack of good breast stimulation. As a basic rule when picking a shield look for the smallest size which is comfortable for you. An IBCLC can help you with determining if there is an issue with sizing. Do not expect that your nipple should extend to the end of the shield when you first put it on - it should be quite a bit longer. Your nipple extends to about twice the normal length while feeding.
Attaching a Shield to the breast
A baby's instincts are to try to grab the breast with their hands when trying to latch on, but they can be quite uncoordinated, particularly if they are not in a laid back position. If you simply set the shield on top of the nipple, it is very likely to be knocked off by waving hands, so vacuuming the shield to the breast can help. There are a couple of ways to do this.
1. Turn the shield half way inside out. Then place the nipple part directly over your nipple. Press in around the base of the nipple so that the rest of the shield folds down against the breast pulling the nipple further into the shield with the vacuum.
2. Hold the outer brim parts of the shields with 2 hands, pull apart to stretch the shield. Then place it over the nipple and breast and release the tension. As the shield moves back into normal position it should pull the nipple further into the shield with the vacuum.
Some people find it helps to moisten the edges of the shield brim to help it to stick.
Cleaning
A shield should be washed with hot soapy water after a feed and rinsed well. If there is thrush present, then Riordan & Wambach (2010) recommend that it should be boiled after use.

Image from Wikipedia - https://commons.wikimedia.org/wiki/File:Placing_shield.jpg

Image from wikipedia - https://commons.wikimedia.org/wiki/Category:Nipple_shields#/media/File:Placed_shield2.jpg
Latching, Feeding and Weaning from the Shield
There is no doubt that many people do find that shields help them to continue feeding when they have hit a rough patch or are having problems getting started, and that the vast majority of people do wean from the shields again later. Some find that easier than others. In my experience one of the things which helps with weaning later is doing your breast to ensure that your baby latches deeply and well to the shield with a nice wide gape. It is very easy when using a shield, to just pop the nipple into a half open mouth and allow the baby to suck their way on to the breast. Some babies are doing this because they are not able to open wide and get their tongue to the breast, and you may be using the shield to get over this issue until it is resolved, but others are able to open wide but learn that they don't need to with the shield.
When latching on - remember the basics of making sure your baby is against your body and that you want a wide gape. It is harder for babies to latch to a shield in a laid back position in my experience, simply because the silcone nipple is long and more unyielding in shape. So you may need to sit more upright to get baby latched. Bring baby close, tummy against you, offer the nipple just above the upper lip, wait for the widest gape you think your baby makes and then bring your baby directly on to the shield nice and deeply so that they attach to the breast. Your baby's lips should not be around the nipple. You should not see the base of the nipple shield. Their lips should be on the breast, cheeks nicely against the breast.
The flow of milk is different when using a shield. When directly on the breast it is usually nice and obvious when a baby has triggered a letdown and you will probably see a swallow at every suck, or every other suck. It's a very distinctive pattern. When feeding from the shield this may not be as obvious. A shield will slow the flow of milk somewhat because there is a physical barrier and the shield needs to fill before milk comes through the holes. As explored above, the number of holes may vary as well which may affect the speed of flow. With a shield you may not see a pattern of swallowing at every suck. It may remain at a pattern of a swallow every 3 sucks for example. It can be a good idea to have a trained breastfeeding worker (IBCLC or accredited breastfeeding counselor, trained HCP) observe a feed with you and help you to identify whether your baby is feeding well with the shield and is drinking rather than just sucking.
Newborns have a very intense need to suck, and a nipple shield provides a nice firm pressure in the mouth to suck on, whether or not there is milk - much like a dummy. So if there is an issue with a baby not getting enough milk it may not be immediately obvious to you unless you know how to identify good feeding and swallowing. A baby may sleepily suck at the breast, fall asleep, wake and become unsettled, but then seem to suck and be contented at the breast without getting good volumes of milk. If you are using a shield then, it is important that you have support around use of the shield and knowing that your baby is feeding well. Your breasts should be fuller before a feed, softer afterwards, and you should be able to see/hear/identify good sustained swallowing during the feed. You should get plenty of wet (heavy wet) and dirty nappies each day indicating that your baby is drinking plenty of milk, and weight gain should be in normal range.
The first step to weaning from a shield again is to ensure that the original issue that caused the shield to be needed is gone! So if it was due to your baby being premature, you may want to wait until your baby would be 40-42 weeks gestation before removing the shield. If it was due to a disorganised suck or tongue tie - has that now been resolved? If it was due to sore nipples, have they now healed enough that you feel comfortable with trying without the shield. Next step is careful positioning & attachment. Talk to an IBCLC or breastfeeding counsellor to help you with this to get the deepest attachment that you can. Usually in the early months this is all that is needed to remove the shield. If the baby still cannot latch you may want to try breast shaping to try to make a narrower shape like the shield, or even to try some nipple manipulation to try to make your nipple more evert. If this isn't working you can latch with the shield, wait till your baby is happily feeding and drinking and then try removing the shield and latching back on. Some babies will latch better when sleepy, or just waking up when they are just acting on instinct. If those things aren't working, talk to an IBCLC for some help.
Removing shields entirely may require a little transition. You may find that at some feeds your baby can do it easily and feeds well. At other feeds they seem to keep losing the latch or just are struggling a little. That's ok. Allow the time. A shield does some of the work that the tongue needs to do otherwise and the baby may need some practice and strength building. You may need to just phase them out over a few days or a couple of weeks.
Pulling it All Together
Nipple shields are a tool and can be a useful tool if used appropriately, feeding/weight gain is monitored and are removed when ready. For me, something like engorgement is usually not a reason I would consider shields, but prematurity / tongue tie / sore nipples where mum is dreading putting her baby to the breast absolutely are reasons I would consider and may suggest shields. Working with an IBCLC / someone who is skilled in breastfeeding support should be able to help you determine if they might be helpful for your situation. I think it is vital that person then watches a feed with you to determine whether your baby is feeding well (attached deeply to the breast, is swallowing plenty of milk) and helps you to identify when your baby is feeding well - since it may look a little different in sucking/swallowing pattern. Weight gain should absolutely be monitored for a week or 2, so that you can start to feel confident that your baby is drinking, and you can start to feel a nice pattern of fuller and emptier breasts. Keeping an eye on wet and dirty nappies is also helpful. Removal is about readiness. For me - that is not all about physical readiness, it is also about psychological readiness. Ideally you want to use shields for a short time and once the issue is resolved, you remove them - but if they are working for you, your baby is feeding well and you are happy using shields, then how you feel about them, and how you feel about removing them is part of the consideration. Nipple shields may have been the thing that saved breastfeeding for you. They may have been the thing which changed a very painful situation into something enjoyable and you may be worried about removing them. Some studies refer to this as dependence. I think this is unhelpful. If breastfeeding has been continued for even a few days or weeks due to the use of shields, if a baby has been able to get breastmilk for longer by using shields, this is a big plus to me. I don't think that being purist about it is helpful. If you never feel ready but your baby is feeding well and you are happy - there isn't really any need to fix what aint broke. On the other hand you may never be happy with using the shields, feel annoyed at having to take them with you when you go out and fiddling to put them on in public, and you may be eager to get rid of them as soon as your baby is able. When you are ready - there are lots of ways to transition and the majority of babies move to feeding at the breast easily. The key is support at all stages - appropriate use, monitoring at the start, support around removing. Tools are helpful if used correctly.
If you have any questions about a consultation or would like to arrange to meet, please get in touch.
Further Reading
1. Powers, D., & Tapia, V. B. (2004). Women’s Experiences Using a Nipple Shield. Journal of Human Lactation, 20(3), 327–334. https://doi.org/10.1177/0890334404267214
2. Chertok, (2009). Reexamination of ultra-thin nipple shield use, infant growth and maternal satisfaction. Journal of Clinical Nursing 18(21), 2949-2955 https://doi.org/10.1111/j.1365-2702.2009.02912.x
3. Meier, P. P., Brown, L. P., Hurst, N. M., Spatz, D. L., Engstrom, J. L., Borucki, L. C., & Krouse, A. M. (2000). Nipple Shields for Preterm Infants: Effect on Milk Transfer and Duration of Breastfeeding. Journal of Human Lactation, 16(2), 106–114. https://doi.org/10.1177/089033440001600205
4. Clum, D., & Primomo, J. (1996). Use of a Silicone Nipple Shield with Premature Infants. Journal of Human Lactation, 12(4), 287–290. https://doi.org/10.1177/089033449601200413
5. Chertok, I., Schneider, J., Blackburn, S. (2006) A Pilot Study of Maternal and Term Infant Outcomes Associated With Ultrathin Nipple Shield Use. Journal of Obstetric, Gynaecological & Neonatal Nursing, 35(2), 265-272. https://doi.org/10.1111/j.1552-6909.2006.00028.x
6. (1987) Serum Prolactin and Cortisol Levels After Suckling for Varying Periods of Time and the Effect of a Nipple Shield, Acta Obstetricia et Gynecologica Scandinavica, 66:1, 47-51, DOI: 10.3109/00016348709092953
7. Bodley, V., & Powers, D. (1996). Long-Term Nipple Shield Use — A Positive Perspective. Journal of Human Lactation, 12(4), 301–304. https://doi.org/10.1177/089033449601200416
8. Kronberg, H., Foverskov, E., Nilsson, I., Maastrup, R., (2016). Why do mothers use nipple shields and how does this influence duration of exclusive breastfeeding. Maternal & Child Nutrition, 13(1) https://doi.org/10.1111/mcn.12251
9. Riordan & Wambach (2010) Breastfeeding & Human Lactation, 4th Ed. Jones & Bartlett Publishers
10. Mohrbacher, N (2010) Breastfeeding Answers Made Simple, A Guide for Helping Mothers. Hale Publishing
Important Information
All material on this website is provided for educational purposes only. Online information cannot replace an in-person consultation with a qualified, independent International Board Certified Lactation Consultant (IBCLC) or your health care provider. If you are concerned about your health, or that of your child, consult with your health care provider regarding the advisability of any opinions or recommendations with respect to your individual situation.